
An encouraging 88% of patients on CALQUENCE remained free of disease progression after 12 months, vs. 68% of patients on rituximab combined with idelalisib or bendamustine
An encouraging 88% of patients on CALQUENCE remained free of disease progression after 12 months, vs. 68% of patients on rituximab combined with idelalisib or bendamustine
WILMINGTON, Del.--(BUSINESS WIRE)-- AstraZeneca today announced detailed results from the interim analysis of the Phase III ASCEND trial at the European Hematology Association (EHA) Annual Congress in Amsterdam, showing CALQUENCE® (acalabrutinib) significantly prolonged the time patients lived without disease progression in relapsed or refractory chronic lymphocytic leukemia (CLL).
This press release features multimedia. View the full release here: https://www.businesswire.com/news/home/20190615005011/en/
The ASCEND trial compared CALQUENCE with the investigator’s choice of rituximab combined with idelalisib (IdR) or bendamustine (BR) in patients with relapsed or refractory CLL.
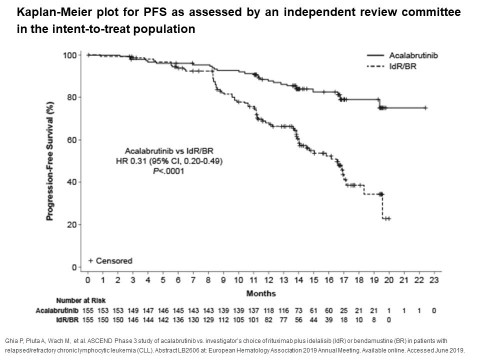
At a median follow-up of 16.1 months, results from the trial showed a statistically-significant and clinically-meaningful improvement in progression-free survival (PFS) for patients treated with CALQUENCE vs. IdR or BR, reducing the risk of disease progression or death by 69% (HR, 0.31: 95% CI, 0.20-0.49, p<0.0001). The median time without disease progression or death for patients treated with CALQUENCE has not yet been reached vs. 16.5 months in the control arm. At 12 months, 88% of patients on CALQUENCE showed no disease progression compared to 68% for the control arm. The safety and tolerability of CALQUENCE was consistent with its established profile.
José Baselga, Executive Vice President, Oncology R&D said: “These data add to the growing body of evidence to support the profile of CALQUENCE as a selective BTK inhibitor that offers a chemotherapy-free treatment option with a favorable safety profile in chronic lymphocytic leukemia, a life-threatening disease. These data, along with our recent positive results from the Phase III ELEVATE-TN trial in previously-untreated chronic lymphocytic leukemia, will serve as the foundation for regulatory submissions later this year.”
Paolo Ghia, MD, Professor, Medical Oncology, Università Vita-Salute San Raffaele in Milan, and investigator of the ASCEND trial, said: “This is the first randomized study to directly compare a BTK inhibitor as monotherapy with standard chemoimmunotherapy or idelalisib and rituximab combinations. With a significant improvement in progression-free survival and a favorable safety profile, acalabrutinib may become an important choice for the treatment of patients with relapsed or refractory chronic lymphocytic leukemia.”
|
Safety overview: |
|||||||||||||
| Most common (≥15%)
AEs, n (%) |
CALQUENCE (N = 154) |
IdR (N = 118) |
BR (N = 35) |
||||||||||
| Any | Grade ≥3 | Any | Grade ≥3 | Any | Grade ≥3 | ||||||||
| Headache | 34 (22%) | 1 (1%) | 7 (6%) | 0 | 0 | 0 | |||||||
| Neutropenia | 30 (19%) | 24 (16%) | 53 (45%) | 47 (40%) | 12 (34%) | 11 (31%) | |||||||
| Diarrhea | 28 (18%) | 2 (1%) | 55 (47%) | 28 (24%) | 5 (14%) | 0 | |||||||
| Anemia | 23 (15%) | 18 (12%) | 11 (9%) | 8 (7%) | 4 (11%) | 3 (9%) | |||||||
| Cough | 23 (15%) | 0 | 18 (15%) | 1 (1%) | 2 (6%) | 0 | |||||||
| Pyrexia | 19 (12%) | 1 (1%) | 21 (18%) | 8 (7%) | 6 (17%) | 1 (3%) | |||||||
| Fatigue | 15 (10%) | 2 (1%) | 10 (8%) | 0 | 8 (23%) | 1(3%) | |||||||
| Nausea | 11 (7%) | 0 | 15 (13%) | 1 (1%) | 7 (20%) | 0 | |||||||
| IRR* | 0 | 0 | 9 (8%) | 2 (2%) | 8 (23%) | 1 (3%) | |||||||
| Events of clinical interest for CALQUENCE | |||||||||||||
| Atrial fibrillation | 8 (5%) | 2 (1%) | 4 (3%) | 1 (1%) | 1 (3%) | 1 (3%) | |||||||
| Bleeding | 40 (26%) | 3 (2%) | 9 (8%) | 3 (3%) | 2 (6%) | 1(3%) | |||||||
| Hypertension | 5 (3%) | 3 (2%) | 5 (4%) | 1 (1%) | 0 | 0 | |||||||
| SPM** excluding NMSC*** | 10 (6%) | 5 (3%) | 3 (3%) | 0 | 1 (3%) | 1 (3%) | |||||||
|
*Infusion related reaction **Secondary primary malignancy ***Non-melanoma skin cancer. |
|||||||||||||
AstraZeneca recently announced that the Phase III ELEVATE-TN trial met its primary endpoint at interim analysis in patients with previously-untreated CLL and that full results will be reported at a forthcoming medical meeting.
IMPORTANT SAFETY INFORMATION ABOUT CALQUENCE (acalabrutinib)
Hemorrhage
Serious hemorrhagic events, including fatal events, have occurred in the combined safety database of 612 patients with hematologic malignancies treated with CALQUENCE monotherapy. Grade 3 or higher bleeding events, including gastrointestinal, intracranial, and epistaxis, have been reported in 2% of patients. Overall, bleeding events, including bruising and petechiae of any grade, occurred in approximately 50% of patients with hematological malignancies.
The mechanism for the bleeding events is not well understood.
CALQUENCE may further increase the risk of hemorrhage in patients receiving antiplatelet or anticoagulant therapies, and patients should be monitored for signs of bleeding.
Consider the benefit-risk of withholding CALQUENCE for 3 to 7 days pre- and post-surgery, depending upon the type of surgery and the risk of bleeding.
Infection
Serious infections (bacterial, viral, or fungal), including fatal events and opportunistic infections, have occurred in the combined safety database of 612 patients with hematologic malignancies treated with CALQUENCE monotherapy. Grade 3 or higher infections occurred in 18% of these patients. The most frequently reported Grade 3 or 4 infection was pneumonia. Infections due to hepatitis B virus (HBV) reactivation and progressive multifocal leukoencephalopathy (PML) have occurred.
Monitor patients for signs and symptoms of infection and treat as medically appropriate. Consider prophylaxis in patients who are at increased risk for opportunistic infections.
Cytopenias
In the combined safety database of 612 patients with hematologic malignancies, patients treated with CALQUENCE monotherapy experienced Grade 3 or 4 cytopenias, including neutropenia (23%), anemia (11%), and thrombocytopenia (8%), based on laboratory measurements. Monitor complete blood counts monthly during treatment.
Second Primary Malignancies
Second primary malignancies, including non-skin carcinomas, have occurred in 11% of patients with hematologic malignancies treated with CALQUENCE monotherapy in the combined safety database of 612 patients. The most frequent second primary malignancy was skin cancer, reported in 7% of patients. Advise protection from sun exposure.
Atrial Fibrillation and Flutter
In the combined safety database of 612 patients with hematologic malignancies treated with CALQUENCE monotherapy, atrial fibrillation and atrial flutter of any grade occurred in 3% of patients, and Grade 3 in 1% of patients. Monitor for atrial fibrillation and atrial flutter and manage as appropriate.
ADVERSE REACTIONS
The most common adverse reactions (≥20%) of any grade were anemia,* thrombocytopenia,* headache (39%), neutropenia,* diarrhea (31%), fatigue (28%), myalgia (21%), and bruising (21%).
*Treatment-emergent decreases (all grades) of hemoglobin (46%), platelets (44%), and neutrophils (36%) were based on laboratory measurements and adverse reactions.
The most common Grade ≥ 3 non-hematological adverse reaction (reported in at least 2% of patients) was diarrhea (3.2%).
Dosage reductions or discontinuations due to any adverse reaction were reported in 1.6% and 6.5% of patients, respectively.
Increases in creatinine 1.5 to 3 times the upper limit of normal occurred in 4.8% of patients.
DRUG INTERACTIONS
Strong CYP3A Inhibitors: Avoid co-administration with a strong CYP3A inhibitor. If a strong CYP3A inhibitor will be used short-term, interrupt CALQUENCE.
Moderate CYP3A Inhibitors: When CALQUENCE is co-administered with a moderate CYP3A inhibitor, reduce CALQUENCE dose to 100 mg once daily.
Strong CYP3A Inducers: Avoid co-administration with a strong CYP3A inducer. If a strong CYP3A inducer cannot be avoided, increase the CALQUENCE dose to 200 mg twice daily.
Gastric Acid Reducing Agents: If treatment with a gastric acid reducing agent is required, consider using an H2-receptor antagonist or an antacid. Take CALQUENCE 2 hours before taking an H2-receptor antagonist. Separate dosing with an antacid by at least 2 hours.
Avoid co-administration with proton pump inhibitors. Due to the long-lasting effect of proton pump inhibitors, separation of doses may not eliminate the interaction with CALQUENCE.
SPECIFIC POPULATIONS
There is insufficient clinical data on CALQUENCE use in pregnant women to inform a drug-associated risk for major birth defects and miscarriage. Advise women of the potential risk to a fetus.
It is not known if CALQUENCE is present in human milk. Advise lactating women not to breastfeed while taking CALQUENCE and for at least 2 weeks after the final dose.
Please see complete Prescribing Information including Patient Information.
– ENDS –
NOTES TO EDITORS
About ASCEND
ASCEND (ACE-CL-309) is a global, randomized, multicenter, open-label Phase III trial evaluating the efficacy of CALQUENCE in previously-treated patients with CLL.2 In the trial, 310 patients were randomized (1:1) into two arms. Patients in the first arm received CALQUENCE monotherapy (100mg twice daily until disease progression). Patients in the second arm received investigator’s choice of either rituximab in combination with idelalisib or rituximab in combination with bendamustine.1,2
The primary endpoint is PFS assessed by an independent review committee (IRC), and key secondary endpoints include investigator-assessed PFS, IRC- and investigator-assessed overall response rate (ORR) and duration of response (DOR), as well as overall survival (OS), patient reported outcomes (PROs) and time to next treatment (TTNT).1,2
About CALQUENCE
CALQUENCE® (acalabrutinib) was granted accelerated approval by the US Food and Drug Administration (FDA) in October 2017 for the treatment of adult patients with MCL who have received at least one prior therapy. Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials.
CALQUENCE is an inhibitor of Bruton tyrosine kinase (BTK). CALQUENCE binds covalently to BTK, thereby inhibiting its activity.3 In B-cells, BTK signaling results in activation of pathways necessary for B-cell proliferation, trafficking, chemotaxis, and adhesion.
As part of an extensive clinical development program, AstraZeneca and Acerta Pharma are currently evaluating CALQUENCE in 26 clinical trials that are company sponsored. CALQUENCE is being developed for the treatment of multiple B-cell blood cancers including CLL, MCL, diffuse large B-cell lymphoma, Waldenstrom macroglobulinemia, follicular lymphoma, and multiple myeloma and other blood cancers. Beyond the positive Phase III clinical trials ASCEND and ELEVATE-TN, other Phase III trials in CLL are ongoing, including ELEVATE-RR (ACE-CL-006) evaluating acalabrutinib vs. ibrutinib in previously treated high-risk CLL and ACE-CL-311 evaluating acalabrutinib in combination with venetoclax and with/without obinutuzumab with previously-untreated CLL without 17p deletion or TP53 mutation.
About chronic lymphocytic leukemia (CLL)
Chronic lymphocytic leukemia (CLL) is the most common type of leukemia in adults, with an estimated 191,000 new cases globally and 20,720 new cases in the US annually, and prevalence that is expected to grow with improved treatment.4-7 In CLL, too many blood stem cells in the bone marrow become abnormal lymphocytes and these abnormal cells have difficulty fighting infections.4 As the number of abnormal cells grows there is less room for healthy white blood cells, red blood cells and platelets.4 This could result in anemia, infection and bleeding.4 B-cell receptor signaling through BTK is one of the essential growth pathways for CLL.
About AstraZeneca in hematology
Leveraging its strength in oncology, AstraZeneca has established hematology as one of four key oncology disease areas of focus. The Company’s hematology franchise includes two US FDA-approved medicines and a robust global development program for a broad portfolio of potential blood cancer treatments. Acerta Pharma serves as AstraZeneca’s hematology research and development arm. AstraZeneca partners with like-minded science-led companies to advance the discovery and development of therapies to address unmet need.
In October 2018, AstraZeneca and Innate Pharma announced a global strategic collaboration that included Innate Pharma licensing the US commercial rights of LUMOXITI™ (moxetumomab pasudotox-tdfk), and with support from AstraZeneca, will continue EU development and commercialization, pending regulatory submission and approval.
About AstraZeneca in oncology
AstraZeneca has a deep-rooted heritage in Oncology and offers a quickly-growing portfolio of new medicines that has the potential to transform patients’ lives and the Company’s future. With at least six new medicines to be launched between 2014 and 2020, and a broad pipeline of small molecules and biologics in development, we are committed to advance Oncology as a key growth driver for AstraZeneca focused on lung, ovarian, breast and blood cancers. In addition to our core capabilities, we actively pursue innovative partnerships and investments that accelerate the delivery of our strategy as illustrated by our investment in Acerta Pharma in hematology.
By harnessing the power of four scientific platforms – Immuno-Oncology, Tumor Drivers and Resistance, DNA Damage Response and Antibody Drug Conjugates – and by championing the development of personalized combinations, AstraZeneca has the vision to redefine cancer treatment and one day eliminate cancer as a cause of death.
About AstraZeneca
AstraZeneca is a global, science-led biopharmaceutical company that focuses on the discovery, development and commercialization of prescription medicines, primarily for the treatment of diseases in three therapy areas - Oncology, Cardiovascular, Renal & Metabolism and Respiratory. AstraZeneca operates in over 100 countries and its innovative medicines are used by millions of patients worldwide. For more information, please visit www.astrazeneca-us.com and follow us on Twitter @AstraZenecaUS.
References
1 Ghia P, Pluta A, Wach M, et al. ASCEND Phase 3 study of acalabrutinib vs. investigator’s choice of rituximab plus idelalisib (IdR) or bendamustine (BR) in patients with relapsed/refractory chronic lymphocytic leukemia (CLL). Abstract LB2606 at: European Hematology Association 2019 Annual Meeting. Available online. Accessed June 2019.
2 ClinicalTrials.gov. A Study of Acalabrutinib vs Investigator's Choice of Idelalisib Plus Rituximab or Bendamustine Plus Rituximab in R/R CLL. NCT02970318. Available online. Accessed June 2019.
3 CALQUENCE® (acalabrutinib) Prescribing Information. AstraZeneca Pharmaceuticals LP, Wilmington, DE.
4 National Cancer Institute. Chronic Lymphocytic Leukemia Treatment (PDQ®)–Patient Version. Available online. Accessed June 2019.
5 Global Burden of Disease Cancer Collaboration. JAMA Oncol. 2017;3(4):524-528.
6 National Institute of Health SEER Program. Cancer Stat Facts: Leukemia—Chronic Lymphocytic Leukemia (CLL). Available online. Accessed June 2019.
7 Jain N, et al. Prevalence and Economic Burden of Chronic Lymphocytic Leukemia (CLL) in the Era of Oral Targeted Therapies. Blood. 2015;126:871.
US-28693 Last Updated 5/19
View source version on businesswire.com: https://www.businesswire.com/news/home/20190615005011/en/
Contacts
Media Inquiries
Michele Meixell +1 302 885 2677
Stephanie Wiswall +1 302 885 2677
Source: AstraZeneca
Smart Multimedia Gallery

View this news release and multimedia online at:
http://www.businesswire.com/news/home/20190615005011/en



