Mesoblast Limited, global leader in allogeneic cellular medicines for inflammatory diseases, announced results from the Phase 3 randomized controlled trial of its allogeneic mesenchymal precursor cell therapy rexlemestrocel-L in 404 enrolled patients with chronic low back pain due to degenerative disc disease refractory to conventional treatments.
NEW YORK, Feb. 10, 2021 (GLOBE NEWSWIRE) -- Mesoblast Limited (Nasdaq:MESO; ASX:MSB), global leader in allogeneic cellular medicines for inflammatory diseases, today announced results from the Phase 3 randomized controlled trial of its allogeneic mesenchymal precursor cell (MPC) therapy rexlemestrocel-L in 404 enrolled patients with chronic low back pain (CLBP) due to degenerative disc disease (DDD) refractory to conventional treatments. The results indicate that a single injection of rexlemestrocel-L may provide a safe, durable, and effective opioid-sparing therapy for patients with chronic inflammatory back pain due to degenerative disc disease, and that greatest benefits are seen when administered earlier in the disease process before irreversible fibrosis of the intervertebral disc has occurred.
“The durable pain reduction for at least two years from a single administration indicates that rexlemestrocel-L has the potential to change the treatment paradigm for chronic low back pain due to inflammatory disc disease, a condition that affects as many as seven million patients across the United States and Europe, and to prevent or reduce opioid use and dependence,” said Dr. Silviu Itescu, Chief Executive Officer of Mesoblast.
Patients were randomized 1:1:1 to receive a single intra-discal injection of either rexlemestrocel-L using a unit dose of 6 million allogeneic mesenchymal precursor cells (MPCs), with or without hyaluronic acid (HA) carrier, or saline control, and stratified for opioid use at baseline to ensure all three treatment arms were equally represented in this pre-defined population. The study was conducted across 48 sites, predominantly in the United States. In a previous randomized controlled trial in patients with refractory CLBP, up to 80% of whom were taking opioids, a single injection of 6 million MPC + HA carrier significantly reduced CLBP for at least two years, while HA alone was no different than saline.1
The effectiveness of rexlemestrocel-L alone or rexlemestrocel-L + HA through 24 months was evaluated on reduction in pain using Visual Analog Score (VAS) and on disability or function using two measurements, Oswestry Disability Index (ODI) and EuroQoL 5-Dimensional (EQ-5D) Index. Key analyses were performed on the total study population and on the pre-specified subsets of opioid users at baseline and patients with CLBP duration shorter or longer than the median for the whole study population.
Regulatory approval of pharmaceutical agents, such as opioids, in the treatment of chronic pain syndromes generally requires reduction in pain as the primary outcome. In the midst of the opioid epidemic in the United States, the Food and Drug Administration has prioritized a focus on new therapeutics that target both pain reduction and opioid avoidance2, particularly for treating CLBP which accounts for 50% of opioid prescriptions.3-5 In addition to assessing the durability of pain reduction with rexlemestrocel-L treatment, this study evaluated primary outcomes using composite measures of pain reduction together with functional responses to treatment, as well as exploratory composites of pain reduction and functional responses in the context of opioid reduction.
A single injection of MPC + Hyaluronic Acid (HA) carrier resulted in:
- Achievement of significant and durable reductions in CLBP through 24 months across the entire evaluable study population (n=391) compared with saline controls
- Greatest pain reduction observed in the pre-specified population with CLBP of shorter duration than the study median of 68 months (n=194), significantly greater reduction at all time points (1, 3, 6, 12, 18 and 24 months) compared with saline controls
- Significantly greater pain reduction in the pre-specified patient subset of opioid users (n=168) at all time-points compared with saline controls
- Confirmation of durable pain reduction seen with the combination of rexlemestrocel-L + HA in the previous randomized controlled trial, where HA control alone was not significantly different from saline1
- Increased composite outcomes of reduction in pain together with improvement in function in those with CLBP of shorter duration than 68 months, the median for the study; however, the composite outcomes of pain and function did not reach statistical significance across the entire study
- No safety concerns over the 24-month period of follow-up in the entire study population
Importantly, in patients using opioids at baseline, the results showed:
- Significant reduction in opioid use over 24 months in patients treated with MPC + HA, while increased opioid use occurred in saline controls
- Treatment with MPC + HA resulted in nearly four times more opioid users achieving 50% reduction in pain as well as reduction in opioid use by 24 months than those treated with saline
Mesoblast will meet with the FDA to discuss the results from this trial together with the earlier randomized controlled trial of MPC + HA, and potential approval pathways for rexlemestrocel-L + HA as treatment for durable reduction in CLBP due to DDD with opioid sparing activity.
Entire Treated Population of Patients
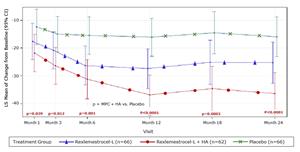
Across the entire treated population in the Phase 3 trial (n=391 evaluable at follow-up), patients who received a single injection of MPC + HA had a significantly greater reduction in pain at both 12 and 24 months compared with saline controls as measured by VAS on a scale of 1-100. Figure 1 shows the least-squared (LS) mean change from baseline in patients treated with MPC + HA was -27.6 at 12 months and -26.0 at 24 months from a baseline mean VAS of 60.4 (p=0.014 and p=0.036, respectively, compared with saline-treated controls). Patients who received MPCs alone had mean VAS reductions intermediate between saline and MPC + HA, indicating an additive role for HA carrier, likely by increasing targeting of mesenchymal stromal cells to inflammatory sites.6 The durable pain reductions observed over 24 months confirm outcomes from a prior randomized controlled trial which showed that the same dose and formulation of MPC + HA resulted in significantly greater reduction in pain, as measured by LS mean change in VAS from baseline, at both 12 months and 24 months compared with saline (p=0.018 and p=0.006, respectively), whereas HA alone was not significantly different from saline.1
Figure 1: LS Mean VAS Low Back Pain Change from Baseline VAS of 60.4 – Entire Study (n=391)
https://www.globenewswire.com/NewsRoom/AttachmentNg/b30efac8-ec8e-4a59-a737-9f22b0bfd402
Maximal pain reduction with MPC + HA was seen in the pre-specified subset of patients treated within a shorter duration of CLBP than the study’s median of 68 months (n=194). Figure 2 shows the least-squared (LS) mean change from baseline in patients treated with MPC + HA was -36.9 at 12 months and -36.5 at 24 months (p<0.0001 at both timepoints compared with saline-treated controls). Further, minimal to no pain (VAS < 20) was seen in 60% of these patients treated with MPC + HA at 12 months and in 54% at 24 months (p=0.011 and p=0.036, respectively, compared to saline controls).
Figure 2: LS Mean VAS Low Back Pain Change from Baseline - Duration CLBP < Median (n=194)
https://www.globenewswire.com/NewsRoom/AttachmentNg/957c024f-2bd7-4a59-a01f-2a953630b265
Pre-specified measurements of function and disability showed that the EuroQoL 5-dimensional questionnaire (EQ-5D) Index appeared to be a more sensitive discriminator of treatment effect than the Oswestry Disability Index (ODI) in this patient population. In the population with shorter duration of CLBP than the median for the study, MPC + HA improved function and disability compared with saline at both 12 and 24 months, as measured by either EQ-5D Index (p=0.009 and p=0.020, respectively) or ODI (p=0.044 and p=0.059, respectively). In these patients MPC + HA resulted in increased composite responder outcomes at 24 months of 50% reduction in pain and improvement in function as measured by either >0.03 EQ-5D Index or by >15-point ODI (p=0.04 and p=0.06, respectively).
Population of Patients Taking Opioids
In the pre-specified population of opioid users at baseline (n=168), patients who received a single injection of MPC + HA had a significantly greater reduction in pain at all time-points (1, 3, 6, 12, 18 and 24 months) compared with saline controls (p<0.05 for all timepoints). Importantly, despite instructions to treating physicians and patients to not change any medications during the trial, by 24 months there was a 40% reduction in opioid use (as measured by morphine equivalent dose, MED) in patients treated with a single injection of MPC + HA (p=0.03). Conversely, more saline treated opioid users actually increased their daily MED opioid use over 24 months than those treated with MPC + HA (50% vs 13% at 24 months, p=0.0009).
By 24 months, 46% of patients treated with MPC + HA achieved 50% reduction in VAS together with opioid MED dose reduction compared with only 12% of saline controls (p=0.004), and 32% vs 12% (p=0.05) achieved a composite of 50% reduction in VAS and 15-point improvement in ODI together with opioid reduction. Treatment with MPC + HA resulted in a 5-fold increase in the proportion of patients achieving a composite of 50% reduction in pain and an EQ-5D Index response at both 12 and 24 months (33% vs 6%, p=0.006) while at the same time reducing opioid use.
Mesoblast Chief Medical Officer Dr. Fred Grossman said: “These results show very meaningful improvements in debilitating CLBP for at least two years after a single injection of our anti-inflammatory mesenchymal precursor cells (MPCs) in an outpatient procedure. On the basis of the Phase 3 trial results, we intend to meet with the FDA and discuss potential pathways towards approval for rexlemestrocel-L, including as an opioid sparing treatment in patients with DDD.”
Conference Call
The archived webcast will be available on the Investor page of the Company’s website: www.mesoblast.com
About Chronic Low Back Pain due to Degenerative Disc Disease
Chronic low back pain (CLBP) affects approximately 10-15% of the adult population, equivalent to more than 30 million people in the United States and almost 40 million people across the EU53. Degenerative disc disease (DDD) causing discogenic pain is the most common etiology of CLBP in adults.7,8 Over 7 million patients in each of the United States and E.U.5 are thought to suffer from CLBP caused by degenerative disc disease,7-9 a disease which involves inflammation and degeneration of the intervertebral discs due to various factors including age, trauma or genetic pre-disposition.
Back pain causes more disability than any other condition9 and inflicts substantial direct and indirect costs on the healthcare system9, including excessive use of opioids in this patient population. There are few treatment options for patients with CLBP who fail conservative therapy, including opioids, spinal injections and surgery (e.g., spinal fusion or total disk arthroplasty).10 More than 50% of US opioid prescriptions are for the treatment of CLBP,3-5 despite the fact that opioids are associated with serious and potentially life-threatening side effects and have not demonstrated efficacy in the treatment of CLBP.5,11,12 In 2018, more than 67,000 drug overdose deaths occurred in the United States13 of which almost 47,000 (70%) were opioid related.
About Mesoblast
Mesoblast is a world leader in developing allogeneic (off-the-shelf) cellular medicines for the treatment of severe and life-threatening inflammatory conditions. The Company has leveraged its proprietary mesenchymal lineage cell therapy technology platform to establish a broad portfolio of late-stage product candidates which respond to severe inflammation by releasing anti-inflammatory factors that counter and modulate multiple effector arms of the immune system, resulting in significant reduction of the damaging inflammatory process.
Mesoblast has a strong and extensive global intellectual property portfolio with protection extending through to at least 2040 in all major markets. The Company’s proprietary manufacturing processes yield industrial-scale, cryopreserved, off-the-shelf, cellular medicines. These cell therapies, with defined pharmaceutical release criteria, are planned to be readily available to patients worldwide.
Mesoblast has completed Phase 3 trials of rexlemestrocel-L for advanced chronic heart failure and chronic low back pain. Remestemcel-L is being developed for inflammatory diseases in children and adults including steroid refractory acute graft versus host disease and moderate to severe acute respiratory distress syndrome. Two products have been commercialized in Japan and Europe by Mesoblast’s licensees, and the Company has established commercial partnerships in Europe and China for certain Phase 3 assets.
Mesoblast has locations in Australia, the United States and Singapore and is listed on the Australian Securities Exchange (MSB) and on the Nasdaq (MESO). For more information, please see www.mesoblast.com, LinkedIn: Mesoblast Limited and Twitter: @Mesoblast
References
- Amirdelfan K, Bae H, et al. Allogeneic mesenchymal precursor cells treatment for chronic low back pain associated with degenerative disc disease: a prospective randomized, placebo-controlled 36-month study of safety and efficacy. The Spine Jnl. 2021;21(2):212-30
- Centers for Disease Control and Prevention
- Decision Resources: Chronic Pain Report 2015.
- Abdel Shaheed C, Maher CG, Williams KA, Day R, McLachlan AJ. Efficacy, tolerability, and dose-dependent effects of opioid analgesics for low back pain: a systematic review and meta-analysis. JAMA Intern Med 2016;176(7):958–68
- Hudson TJ, Edlund MJ, Steffick DE, Tripathi SP, Sullivan MD. Epidemiology of regular prescribed opioid use: results from a national, population-based survey. J Pain Symptom Manage 2008;36(3):280–8
- Corradetti B, et al. Hyaluronic acid coatings as a simple and efficient approach to improve MSC homing toward the site of inflammation. Nature – Scientific Reports 2017;7:7991
- DePalma MJ, et al. What Is the Source of Chronic Low Back Pain and Does Age Play a Role? Pain Med. 2011; 12: 224–233
- Peng BG. Pathophysiology, diagnosis, and treatment of discogenic low back pain. World J Orthop. 2013 April 18; 4(2): 42-52
- Williams, J., NG, Nawi, Pelzter, K. (2015) Risk factors and disability associated with low back pain in older adults in low-and middle-income countries. Results from the WHO Study on global ageing and adult health (SAGE). PloS One. 2015; 10(6): e0127880
- Zigler J, et al. Comparison of lumbar total disc replacement with surgical spinal fusion for the treatment of single-level degenerative disc disease: a meta-analysis of 5-year outcomes from randomized controlled trials. Glob Spine J. 2018;8(4):413–23
- Chaparro LE, Furlan AD, Deshpande A, Mailis-Gagnon A, Atlas S, Turk DC. Opioids compared to placebo or other treatments for chronic low-back pain. Cochrane Database Syst Rev 2013(8):CD004959
- Chou R, Turner JA, Devine EB, Hansen RN, Sullivan SD, Blazina I, et al. The effectiveness and risks of long-term opioid therapy for chronic pain: a systematic review for a National Institutes of Health Pathways to Prevention Workshop. Ann Intern Med 2015;162 (4):276–86
- Annual surveillance report of drug-related risks and outcomes United States, 2019. Centers for Disease Control and Prevention
Forward-Looking Statements
This announcement includes forward-looking statements that relate to future events or our future financial performance and involve known and unknown risks, uncertainties and other factors that may cause our actual results, levels of activity, performance or achievements to differ materially from any future results, levels of activity, performance or achievements expressed or implied by these forward-looking statements. All statements other than statements of historical fact, including our intention to discuss potential pathways to potential approval with the FDA, are forward-looking statements, which are often indicated by terms such as “anticipate,” “believe,” “could,” “estimate,” “expect,” “goal,” “intend,” “likely,” “look forward to,” “may,” “plan,” “potential,” “predict,” “project,” “should,” “will,” “would” and similar expressions and variations thereof. We make such forward-looking statements pursuant to the safe harbor provisions of the Private Securities Litigation Reform Act of 1995 and other federal securities laws. Forward-looking statements should not be read as a guarantee of future performance or results, and actual results may differ from the results anticipated in these forward-looking statements, and the differences may be material and adverse. The risks, uncertainties and other factors that may impact our forward-looking statements include, but are not limited to: the commencement, timing, progress and results of Mesoblast’s or its partner’s preclinical and clinical studies; Mesoblast’s or its partner’s ability to advance product candidates into, enroll and successfully complete, clinical studies; the timing or likelihood of regulatory filings and approvals; whether the FDA agrees to a potential approval pathway; and the pricing and reimbursement of Mesoblast’s or its partner’s product candidates, if approved; Mesoblast’s ability to establish and maintain intellectual property on its product candidates and Mesoblast’s ability to successfully defend these in cases of alleged infringement. You should read this press release together with our risk factors, in our most recently filed reports with the SEC or on our website. Uncertainties and risks that may cause Mesoblast’s actual results, performance or achievements to be materially different from those which may be expressed or implied by such statements, and accordingly, you should not place undue reliance on these forward-looking statements. Unless required by law, we do not undertake any obligations to publicly update or revise any forward-looking statements, whether as a result of new information, future developments or otherwise.
Release authorized by the Chief Executive.
For more information, please contact:
| Corporate Communications / Investors | |
| Schond Greenway T: +1 212 880 2060 E: schond.greenway@mesoblast.com |
Paul Hughes T: +61 3 9639 6036 E: paul.hughes@mesoblast.com |
| Media Kristen Bothwell T: +1 917 613 5434 E:kbothwell@rubenstein.com |
|
![]()
LS Mean VAS Low Back Pain Change from Baseline VAS of 60.4 – Entire Study (n=391)
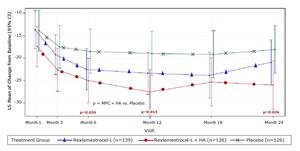
Figure 1
LS Mean VAS Low Back Pain Change from Baseline - Duration CLBP < Median (n=194)