BioDelivery Sciences International, Inc. (NASDAQ: BDSI), today presented at the American Academy of Pain Medicine’s 36th Annual Meeting.
BELBUCA® Effect on Respiratory Drive was Comparable to Placebo in Clinical Trial at all Tested Doses
Immediate Release Oral Oxycodone HCl Associated with a Dose-Dependent Decrease in Respiratory Drive Compared to Placebo
RALEIGH, N.C., Feb. 27, 2020 (GLOBE NEWSWIRE) -- BioDelivery Sciences International. (NASDAQ: BDSI), a rapidly growing specialty pharmaceutical company dedicated to patients living with serious and complex chronic conditions, today presented at the American Academy of Pain Medicine’s (AAPM) 36th Annual Meeting the results of a study titled, “A Phase I Placebo-Controlled Trial Comparing the Effect of Buprenorphine Buccal Film and Oral Oxycodone Hydrochloride on Respiratory Drive”.
In May 2019, in response to significant challenges chronic pain patients face in obtaining adequate care and the ongoing opioid crisis, The Pain Management Best Practices Inter-Agency Task Force report recommended more research activities directed to better understanding the use of buprenorphine, a Schedule III opioid. Opioids can cause serious, life-threatening, or fatal respiratory depression. Respiratory depression is a breathing disorder characterized by slow and ineffective breathing and is the leading cause of opioid related deaths. In this clinical trial, BDSI evaluated the effect of BELBUCA® (buprenorphine buccal film), a Schedule III opioid, and oral oxycodone HCI, a Schedule II opioid, on respiratory drive.
Study Design:
– Study subjects (N = 19) were healthy males and females self-identifying as recreational drug users and determined via naloxone challenge to not be physically dependent on opioids.
– Effect on respiratory drive was assessed using a double-blind, double-dummy, 6-treatment, 6-period, placebo controlled, randomized crossover design.
– Treatments studied included single doses of: BELBUCA (300 mcg, 600 mcg, and 900 mcg); oral oxycodone hydrochloride (Oxy 30 mg and 60 mg); and placebo (each separated by a 7-day washout period).
– Respiratory drive was evaluated by measuring the ventilatory response to hypercapnia (excess carbon dioxide in the bloodstream) through assessment of the maximum change in minute ventilation (Emax), which is the maximum amount inhaled or exhaled in one minute, after administration of each study drug. Statistical analyses were performed using a linear mixed-effects model.
Results:
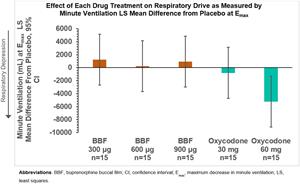
– The least square mean differences in Emax versus placebo were as follows: Oxy 30 mg (−828.5, P=0.668); Oxy 60 mg (−5188.6, P=0.008); BELBUCA 300 mcg (+1206.9, P=0.533); BELBUCA 600 mcg (+245.4, P=0.896); and BELBUCA 900 mcg (+1473.3, P=0.440).
A chart/graphic accompanying this announcement is available at:
https://www.globenewswire.com/NewsRoom/AttachmentNg/d148dcf8-f359-4b36-ada6-dd34da39f6e6
Conclusion:
– BELBUCA effect on respiratory drive was comparable to placebo at all doses tested.
– The effect of immediate release oral oxycodone HCl resulted in a dose-dependent decrease in respiratory drive compared to placebo.
“This is an important and novel study that shows the comparative effects of buprenorphine buccal film and oral oxycodone on respiratory drive,” stated Lynn Webster, M.D., the principal investigator of the study. Thomas Smith, M.D., Chief Medical Officer at BDSI, added, “Consistent with the Task Force’s recommendation, BDSI is providing the medical community with the results of this safety study to help providers make informed treatment decisions. This study provides additional scientific support for the use of BELBUCA as a primary treatment option for the management of pain severe enough to require daily, around-the-clock, long-term opioid treatment and for which alternative treatment options are inadequate.”
Serious, life-threatening, or fatal respiratory depression may occur with use of BELBUCA. BELBUCA is contraindicated in patients with significant respiratory depression; acute or severe bronchial asthma in an unmonitored setting or in the absence of resuscitative equipment; known or suspected gastrointestinal obstruction, including paralytic ileus; and hypersensitivity (e.g., anaphylaxis) to buprenorphine.
Please see important safety information about BELBUCA below.
For full Prescribing Information, including Boxed Warning, visitwww.belbuca.com.
The Pain Management Best Practices Inter-Agency Task Force report is available for viewing online at https://www.hhs.gov/ash/advisory-committees/pain/index.html.
IMPORTANT SAFETY INFORMATION ABOUT BELBUCA®
INDICATION
BELBUCA® (buprenorphine buccal film) is indicated for the management of pain severe enough to require daily, around-the-clock, long-term opioid treatment and for which alternative treatment options are inadequate.
Limitations of Use
- Because of the risks of addiction, abuse, and misuse with opioids, even at recommended doses, and because of the greater risks of overdose and death with long-acting opioid formulations, reserve BELBUCA for use in patients for whom alternative treatment options (e.g., non-opioid analgesics or immediate-release opioids) are ineffective, not tolerated, or would be otherwise inadequate to provide sufficient management of pain.
- BELBUCA is not indicated as an as-needed (prn) analgesic.
IMPORTANT SAFETY INFORMATION about BELBUCA®
WARNING: ADDICTION, ABUSE, AND MISUSE; RISK EVALUATION AND MITIGATION STRATEGY (REMS); LIFE-THREATENING RESPIRATORY DEPRESSION; ACCIDENTAL EXPOSURE; NEONATAL OPIOID WITHDRAWAL SYNDROME; and RISKS FROM CONCOMITANT USE WITH BENZODIAZEPINES AND OTHER CNS DEPRESSANTS Addiction, Abuse, and Misuse BELBUCA exposes patients and other users to the risks of opioid addiction, abuse, and misuse, which can lead to overdose and death. Assess each patient’s risk prior to prescribing BELBUCA, and monitor regularly for these behaviors and conditions. Risk Evaluation and Mitigation Strategy (REMS) To ensure that the benefits of opioid analgesics outweigh the risks of addiction, abuse, and misuse, the FDA has required a REMS for these products. Under the requirements of the REMS, drug companies with approved opioid analgesic products must make REMS-compliant education programs available to healthcare providers. Healthcare providers are strongly encouraged to
Serious, life-threatening, or fatal respiratory depression may occur with use of BELBUCA. Monitor for respiratory depression, especially during initiation of BELBUCA or following a dose increase. Misuse or abuse of BELBUCA by chewing, swallowing, snorting, or injecting buprenorphine extracted from the buccal film will result in the uncontrolled delivery of buprenorphine and poses a significant risk of overdose and death. Accidental Exposure Accidental exposure to even one dose of BELBUCA, especially in children, can result in a fatal overdose of buprenorphine. Neonatal Opioid Withdrawal Syndrome Prolonged use of BELBUCA during pregnancy can result in neonatal opioid withdrawal syndrome, which may be life-threatening if not recognized and treated. If prolonged opioid use is required in a pregnant woman, advise the patient of the risk of neonatal opioid withdrawal syndrome and ensure that appropriate treatment will be available. Risks from Concomitant Use with Benzodiazepines Or Other CNS Depressants Concomitant use of opioids with benzodiazepines or other central nervous system (CNS) depressants, including alcohol, may result in profound sedation, respiratory depression, coma, and death. Reserve concomitant prescribing for use in patients for whom alternative treatment options are inadequate; limit dosages and durations to the minimum required; and follow patients for signs and symptoms of respiratory depression and sedation. |
CONTRAINDICATIONS
BELBUCA is contraindicated in patients with significant respiratory depression; acute or severe bronchial asthma in an unmonitored setting or in the absence of resuscitative equipment; known or suspected gastrointestinal obstruction, including paralytic ileus; and hypersensitivity (e.g., anaphylaxis) to buprenorphine.
WARNINGS AND PRECAUTIONS
Addiction, Abuse, and Misuse
- BELBUCA contains buprenorphine, a Schedule III controlled substance. As an opioid, BELBUCA exposes users to the risks of addiction, abuse, and misuse. Although the risk of addiction in any individual is unknown, it can occur in patients appropriately prescribed BELBUCA. Addiction can occur at recommended dosages and if the drug is misused or abused.
- Assess each patient’s risk for opioid addiction, abuse, or misuse prior to prescribing BELBUCA and monitor all patients receiving BELBUCA for the development of these behaviors and conditions. Risks are increased in patients with a personal or family history of substance abuse (including drug or alcohol abuse or addiction) or mental illness (e.g., major depression). The potential for these risks should not, however, prevent the proper management of pain in any given patient. Patients at increased risk may be prescribed opioids such as BELBUCA, but use in such patients necessitates intensive counseling about the risks and proper use of BELBUCA, along with intensive monitoring for signs of addiction, abuse, or misuse.
- Abuse or misuse of BELBUCA by swallowing may cause choking, overdose, and death.
- Opioids are sought by drug abusers and people with addiction disorders and are subject to criminal diversion. Consider these risks when prescribing or dispensing BELBUCA. Strategies to reduce the risk include prescribing the drug in the smallest appropriate quantity and advising the patient on the proper disposal of unused drug.
Opioid Analgesic Risk Evaluation and Mitigation Strategy (REMS)
- To ensure that the benefits of opioid analgesics outweigh the risks of addiction, abuse, and misuse, the FDA has required a REMS for these products. Under the requirements of the REMS, drug companies with approved opioid analgesic products must make REMS-compliant education programs available to healthcare providers. To obtain further information on the REMS and for a list of accredited REMS CME/CE, call 1-800-503-0784, or log on to www.opioidanalgesicrems.com
- Healthcare providers are strongly encouraged to complete a REMS-compliant education program; to discuss the safe use, serious risks, and proper storage and disposal of opioid analgesics with patients or caregivers; to emphasize to patients and caregivers the importance of reading the Medication Guide; and to consider using other tools to improve patient, household, and community safety, such as patient-prescriber agreements that reinforce patient-prescriber responsibilities.
Life-Threatening Respiratory Depression
- Serious, life-threatening, or fatal respiratory depression has been reported with the use of opioids, even when used as recommended. Respiratory depression, if not immediately recognized and treated, may lead to respiratory arrest and death.
- While serious, life-threatening or fatal respiratory depression can occur at any time during the use of BELBUCA, the risk is greatest during initiation of therapy or following a dosage increase. Monitor patients closely for respiratory depression when initiating therapy with BELBUCA and following dosage increases.
- To reduce the risk of respiratory depression, proper dosing and titration of BELBUCA are essential. Overestimating the dose of BELBUCA when converting patients from another opioid product may result in fatal overdose with the first dose.
- Accidental exposure to BELBUCA, especially in children, can result in respiratory depression and death due to an overdose of buprenorphine.
- Opioids can cause sleep-related breathing disorders including central sleep apnea (CSA) and sleep-related hypoxemia. Opioid use increases the risk of CSA in a dose-dependent fashion. In patients who present with CSA, consider decreasing the opioid dosage using best practices for opioid taper.
Neonatal Opioid Withdrawal Syndrome
- Prolonged use of BELBUCA during pregnancy can result in withdrawal in the neonate. Neonatal opioid withdrawal syndrome, unlike opioid withdrawal syndrome in adults, may be life-threatening if not recognized and treated, and requires management according to protocols developed by neonatology experts. Observe newborns for signs of neonatal opioid withdrawal syndrome and manage accordingly. Advise pregnant women using opioids for a prolonged period of the risk of neonatal opioid withdrawal syndrome and ensure that appropriate treatment will be available.
Risks due to Interactions with Benzodiazepines or Other Central Nervous System Depressants
- Profound sedation, respiratory depression, coma, and death may result from the concomitant use of BELBUCA with benzodiazepines or other CNS depressants (e.g., non-benzodiazepine sedatives/hypnotics, anxiolytics, tranquilizers, muscle relaxants, general anesthetics, antipsychotics, other opioids, alcohol). Because of these risks, reserve concomitant prescribing of these drugs for use in patients for whom alternative treatment options are inadequate.
If the decision is made to prescribe a benzodiazepine or other CNS depressant concomitantly with an opioid analgesic, prescribe the lowest effective dosages and minimum durations of concomitant use. Follow patients closely for signs and symptoms of respiratory depression and sedation.
Risk of Life-Threatening Respiratory Depression in Patients with Chronic Pulmonary Disease or in Elderly, Cachectic, or Debilitated Patients
- The use of BELBUCA in patients with acute or severe bronchial asthma in an unmonitored setting or in the absence of resuscitative equipment is contraindicated.
- BELBUCA-treated patients with significant chronic obstructive pulmonary disease or cor pulmonale, and those with substantially decreased respiratory reserve, hypoxia, hypercapnia, or pre-existing respiratory depression are at increased risk of decreased respiratory drive, including apnea, even at recommended dosages of BELBUCA.
- Life-threatening respiratory depression is more likely to occur in elderly, cachectic, or debilitated patients as they may have altered pharmacokinetics or altered clearance compared with younger, healthier patients.
- Monitor such patients closely, particularly when initiating and titrating BELBUCA and when BELBUCA is given concomitantly with other drugs that depress respiration.
Adrenal Insufficiency
- Cases of adrenal insufficiency have been reported with opioid use, more often following greater than one month of use. Presentation of adrenal insufficiency may include non-specific symptoms and signs including nausea, vomiting, anorexia, fatigue, weakness, dizziness, and low blood pressure. If adrenal insufficiency is suspected, confirm the diagnosis with diagnostic testing as soon as possible. If adrenal insufficiency is diagnosed, treat with physiologic replacement doses of corticosteroids. Wean the patient off of the opioid to allow adrenal function to recover and continue corticosteroid treatment until adrenal function recovers. Other opioids may be tried as some cases reported use of a different opioid without recurrence of adrenal insufficiency. The information available does not identify any particular opioids as being more likely to be associated with adrenal insufficiency.
QTc Prolongation
- BELBUCA has been observed to prolong the QTc interval in some subjects participating in clinical trials. Consider these observations in clinical decisions when prescribing BELBUCA to patients with hypokalemia, hypomagnesemia, or clinically unstable cardiac disease, including unstable atrial fibrillation, symptomatic bradycardia, unstable congestive heart failure, or active myocardial ischemia. Periodic electrocardiographic (ECG) monitoring is recommended in these patients. Avoid the use of BELBUCA in patients with a history of Long QT Syndrome or an immediate family member with this condition or those taking Class IA antiarrhythmic medications (e.g., quinidine, procainamide, disopyramide) or Class III antiarrhythmic medications (e.g., sotalol, amiodarone, dofetilide), or other medications that prolong the QT interval.
Severe Hypotension
- BELBUCA may cause severe hypotension including orthostatic hypotension and syncope in ambulatory patients. There is an increased risk in patients whose ability to maintain blood pressure has already been compromised by a reduced blood volume or concurrent administration of certain CNS depressant drugs (e.g., phenothiazines or general anesthetics). Monitor these patients for signs of hypotension after initiating or titrating the dosage of BELBUCA. In patients with circulatory shock, BELBUCA may cause vasodilation that can further reduce cardiac output and blood pressure. Avoid the use of BELBUCA in patients with circulatory shock.
Risks of Use in Patients with Increased Intracranial Pressure, Brain Tumors, Head Injury, or Impaired Consciousness
- In patients who may be susceptible to the intracranial effects of CO2 retention (e.g., those with evidence of increased intracranial pressure or brain tumors), BELBUCA may reduce respiratory drive, and the resultant CO2 retention can further increase intracranial pressure. Monitor such patients for signs of sedation and respiratory depression, particularly when initiating therapy with BELBUCA.
- Opioids may also obscure the clinical course in a patient with a head injury. Avoid the use of BELBUCA in patients with impaired consciousness or coma.
Hepatotoxicity
- Cases of cytolytic hepatitis and hepatitis with jaundice have been observed in individuals receiving sublingual formulations of buprenorphine for the treatment of opioid dependence, both in clinical trials and in post-marketing adverse events reports. For patients at increased risk of hepatotoxicity (e.g., patients with a history of excessive alcohol intake, intravenous drug abuse or liver disease), obtain baseline liver enzyme levels and monitor periodically during treatment with BELBUCA.
Risk of Overdose in Patients with Moderate or Severe Hepatic Impairment
- In a pharmacokinetic study of subjects dosed with buprenorphine sublingual tablets, buprenorphine plasma levels were found to be higher and the half-life was found to be longer in subjects with moderate and severe hepatic impairment, but not in subjects with mild hepatic impairment. For patients with severe hepatic impairment, a dose adjustment is recommended, and patients with moderate or severe hepatic impairment should be monitored for signs and symptoms of toxicity or overdose caused by increased levels of buprenorphine.
Anaphylactic/Allergic Reactions
- Cases of acute and chronic hypersensitivity to buprenorphine have been reported both in clinical trials and in post-marketing experience. The most common signs and symptoms include rashes, hives, and pruritus. Cases of bronchospasm, angioneurotic edema, and anaphylactic shock have been reported.
Withdrawal
- Do not abruptly discontinue BELBUCA in a patient physically dependent on opioids. When discontinuing BELBUCA in a physically dependent patient, gradually taper the dosage. Rapid tapering of buprenorphine in a patient physically dependent on opioids may lead to a withdrawal syndrome and return of pain.
- Additionally, the use of BELBUCA, a partial agonist opioid analgesic, in patients who are receiving a full opioid agonist analgesic may reduce the analgesic effect and/or precipitate withdrawal symptoms. Avoid concomitant use of BELBUCA with a full opioid agonist analgesic.
Risk of Use in Patients with Gastrointestinal Conditions
- BELBUCA is contraindicated in patients with known or suspected gastrointestinal obstruction, including paralytic ileus.
- BELBUCA may cause spasm of the sphincter of Oddi. Opioids may cause increases in the serum amylase. Monitor patients with biliary tract disease, including acute pancreatitis, for worsening symptoms.
Increased Risk of Seizures in Patients with Seizure Disorders
- The buprenorphine in BELBUCA may increase the frequency of seizures in patients with seizure disorders, and may increase the risk of seizures occurring in other clinical settings associated with seizures. Monitor patients with a history of seizure disorders for worsened seizure control during BELBUCA therapy.
Risks of Use in Cancer Patients with Oral Mucositis
- Cancer patients with oral mucositis may absorb buprenorphine more rapidly than intended and are likely to experience higher plasma levels of the opioid. For patients with known or suspected mucositis, a dose reduction is recommended. Monitor these patients carefully for signs and symptoms of toxicity or overdose caused by increased levels of buprenorphine.
Risks of Driving and Operating Machinery
- BELBUCA may impair the mental and physical abilities needed to perform potentially hazardous activities such as driving a car or operating machinery. Warn patients not to drive or operate dangerous machinery unless they are tolerant to side effects of BELBUCA and know how they will react to the medication.
ADVERSE REACTIONS
- The most common adverse reactions (≥5%) reported by patients treated with BELBUCA in the clinical trials were nausea, constipation, headache, vomiting, fatigue, dizziness, and somnolence.
Please see full Prescribing Information, including Boxed Warning and Medication Guide, for BELBUCA.
To report SUSPECTED ADVERSE REACTIONS, contact BioDelivery Sciences International, Inc. at 1-800-469-0261 or FDA at 1-800-FDA-1088 or www.fda.gov/safety/medwatch.
Intended for healthcare professionals of the United States of America only.
About BioDelivery Sciences International, Inc.
BioDelivery Sciences International, Inc. (NASDAQ: BDSI) is a commercial-stage specialty pharmaceutical company dedicated to patients living with chronic conditions. BDSI has built a portfolio of products that includes utilizing its novel and proprietary BioErodible MucoAdhesive (BEMA®) technology to develop and commercialize, either on its own or in partnership with third parties, new applications of proven therapies aimed at addressing important unmet medical needs. BDSI's marketed products address serious and debilitating conditions, including chronic pain, opioid dependence, and opioid-induced constipation.
Cautionary Note on Forward-Looking Statements
This press release and any statements of employees, representatives, and partners of BDSI related thereto contain, or may contain, among other things, certain “forward-looking statements” within the meaning of the Private Securities Litigation Reform Act of 1995. Such forward-looking statements involve significant risks and uncertainties. Such statements may include, without limitation, statements with respect to the BDSI’s plans, objectives, projections, expectations and intentions and other statements identified by words such as “projects,” “may,” “will,” “could,” “would,” “should,” “believes,” “expects,” “anticipates,” “estimates,” “intends,” “plans,” “potential” or similar expressions. These statements are based upon the current beliefs and expectations of the BDSI’s management and are subject to significant risks and uncertainties, including those detailed in the BDSI’s filings with the Securities and Exchange Commission. Actual results may differ materially from those set forth or implied in the forward-looking statements. These forward-looking statements involve certain risks and uncertainties that are subject to change based on various factors (many of which are beyond the BDSI’s control) including those set forth in our 2018 annual report on Form 10-K filed with the US Securities and Exchange Commission and subsequent filings. BDSI undertakes no obligation to publicly update any forward-looking statements, whether as a result of new information, future presentations or otherwise, except as required by applicable law.
© 2020 BioDelivery Sciences International, Inc. All rights reserved.
Contact:
Tirth T. Patel
Director of Investor Relations
tpatel@bdsi.com
(919) 582-0294

Effect of Each Drug Treatment on Respiratory Drive as Measured by Minute Ventilation LS Mean Difference from Placebo at Emax